
An Address on the Hæmatozoa of Malaria
AN ADDRESS ON THE HAEMATOZOA OF MALARIA.[1]
By WILLIAM OSLER, M.D., F.R.C.P
Professor of Clinical Medicine in the University of Pennsylvania.
Our knowledge of the animal parasites infesting the blood has been of late enriched by observations which show that certain of these hæmatozoa, as they are called, are more widely distributed and more important than we had hitherto supposed. Parasites belonging to the spirozoa, and to the nematode and trematode worms, have long been known to occur in the blood of various animals. Recent investigations prove that the flagellate protozoa are also not uncommon blood parasites, and it is possible that they may be the pathogenic organisms of certain diseases. I propose in this communication to give an account of the hæmatozoa which have been found in persons suffering with the various forms of malaria.
Historical.—Our knowledge of the blood-changes I am about to describe, dates from the researches of Laveran, in Algiers, which were communicated to the Paris Academy of Medicine in 1881 and 1882, and which were finally embodied in a large work on the malarial fevers, published in 1884.[2] He found, as characteristic elements in the blood of persons attacked with malaria, (1) crescentic pigmented bodies; (2) pigmented bodies in the interior of the red corpuscles, which underwent changes in form, described as amœboid; and (3) a pigmented flagellate organism. These forms were looked upon as phases in the development of an infusorial organism which he regarded as the germ of the disease. Richard [3] confirmed these observations. A more general interest in the question was aroused by the publications of Marchiafava and Celli,[4] who found in the blood of malarial patients at Rome the bodies described by Laveran. They figured carefully the alterations of the organism in the interior of the red corpuscles to which they gave the name Plasmodium malariæ. Councilman, of Baltimore, has more recently confirmed these observations.[5] The pigment granules so numerous in the interior of the red corpuscles in cases of "comatose pernicious fever," and which appear to be included in a hyaline mass are, according to Marchiafava and Celli, and Councilman (who had previously described them[6]) these amœboid parasites deeply laden with altered hæmoglobin.
Technical Details.—The finger pad from which the blood drop is taken should be thoroughly cleansed, and, if the examination is made during a paroxysm, the sweat which may exude after the friction and drying should be removed. Attention to these, apparently trivial, details will secure specimens of blood free from small particles of dirt, and facilitate considerably the search for pigmented bodies. The layer of blood beneath the top cover should be very thin and uniform, the corpuscles, as far as possible, isolated and not aggregated in clumps or in rouleaux. It is well to surround the cover with paraffin if the examination is prolonged. No reagent of any kind should be added. Cover-glass preparations may be made and stained in methyl blue or fuchsin, and mounted in balsam. Osmic acid preparations may also be employed. Although these bodies may be seen with a power of 500 to 600 diameters, it is essential for the satisfactory study of the changes to use higher powers. I have uniformly worked with the ??? homo. immersion of Zeiss, and the ?? im. of Reichert. Stricker's warm stage will be found useful.
Description of the bodies
1. The Forms which Exist within the Red Corpuscle.—(a) The most common alteration in the blood of malarial patients is presented by a pigmented structure inside the red corpuscle. The attention of the observer will most likely be first attracted by the presence of a few dark grains in the stroma, and a careful study of a suitable specimen will soon lead to the conviction that these are not scattered loosely, but are enclosed in a finely granular or hyaline body in the interior of the corpuscle (Fig. 1). The red discs in which

they occur are usually larger, look flat, and are very often paler than normal; they may, indeed, exist only as colourless shells. The number of corpuscles so affected varies extremely in different cases. In some instances they are readily found after a search of a moment or two, but, in other cases, a prolonged examination may be necessary. Only one is usually present in each corpuscle, but two or three, or even four, may occupy the stroma. They vary greatly in size, the smaller ones not occupying a fourth of the corpuscle, while the larger ones may almost fill it. A delicate contour line can usually be seen separating the body from the stroma; at times this is very indistinct, particularly if the illumination is very bright. The substance appears hyaline, or very finely granular, and the pigment grains are scattered irregularly in it. They may be very numerous, and give a dark aspect to the body, or they may be scanty. They frequently present rapid Brownian movements. Occasionally a vacuole may be seen in the interior of the body. In several instances the bodies appeared to be enclosed in a clear space—vacuole—in the stroma. When first seen they are more or less spherical, but, as already stated, the outline may be indistinct. The pigment granules may be seen to alter their position in relation to each other. If the margin of the body is carefully observed, slow changes can be seen, which gradually bring about alterations in shape. These movements, which appear to be amœboid in character, can often be traced with great ease. They are well represented at Fig.1, and, better still, at Fig.2. Changes in position of the body in the corpuscle result from them. They are decidedly slower than the amœboid movement of the colourless corpuscle. I have not seen any evidence of migration from the corpuscle. In dry preparations
these bodies stain deeply with gentian violet or fuchsin,and present a granular stroma, in which the pigment grains are imbedded. (Fig. 3.)
(b) In seven cases peculiar hyaline structures existed in the interior of the red corpuscles, which differ from the bodies just described, in the absence of pigment and in the much greater activity of the changes. Fig. 4 illustrates the appearance and the alterations in outline. These
bodies are devoid of structure, and the corpuscles in which they are present are not so pale as those with the pigmented forms. Marchiafava and Celli, who have given an excellent plate of these bodies,[7] regard them as the initial forms of the pigmented bodies. One does occasionally see appearances indicative of commencing pigmentation, but they have not, as a rule, the solid aspect of the pigmented bodies. In three cases I have seen the following remarkable changes. The hyaline body, while actively changing shape, suddenly burst from the stroma, and disappeared, or formed only a few granules. Thus, in a red corpuscle, there were, at 3.40 p.m., two hyaline, irregular-shaped bodies, which were changing rapidly in outline. The alterations were so marked that the physicians present at the time had no difficulty in seeing them. The stroma of the corpuscle was of full colour. At 3.50 p.m., as I was carefully watching these forms, the corpuscle suddenly ruptured, and gave exit to two distinct masses, which quickly
broke up into ten or twelve spherical bodies. No change took place in these after twelve hours, except that they became pale and indistinct. The stroma of the corpuscle became quite colourless. On two other occasions a similar phenomenon was witnessed, but in one no trace could be seen of the extruded material. This is evidently a physical change, and I think these very pale hyaline bodies must be carefully distinguished from the pigmented forms, though possibly associated with their early development.
(c) In seven cases there were vacuoles in the red corpuscles containing solid-looking bodies of various sizes and shapes. Certain of these structures resembled micrococci very closely (Fig.5), and stained

deeply in aniline dyes; but others, often in the same corpuscle,were larger, more irregular, and altogether different in appearance (Fig. 6).
The smaller ones were usually highly refractile, and,when two were together, the appearance suggested a diplococcus. In three instances these bodies had a deep brown tint, as if composed of pigment. The larger bodies were homogeneous, very variable in size and shape. No movement was noticed in them, but the outlines of the spaces in which they lay sometimes changed actively. In Case 29, these bodies were very abundant, and for days formed the only noticeable alteration in the corpuscles.
2. The Free Forms.—(a) Pigmented crescents. These bodies, which were found in eighteen cases, present remarkable features in appearance and structure. The form was usually that of a beautiful crescent (Fig.7), with rounded or gently tapering ends; but the degree
of curvature was variable, and many forms were almost straight. The length is about double that of the width of a red corpuscle, sometimes more. They are not attached, and they never show any motion. Joining the ends of the crescents—or, more correctly, at a little distance from the points—a narrow line can often be seen on the concave margin (Fig.7, e). The body of the crescent appears made up of a structureless, homogeneous material, in the centre of which is a prominent collection of pigment granules. This, with the peculiar form, makes these bodies very easily recognisable in the blood, even when closely surrounded by the corpuscles. The pigment is very dark in colour, distinctly granular, and varies somewhat in its arrangement. As a rule, it is central and aggregated, either in a heap, or assumes the form of a band placed transversely to the axis of the crescent. In some instances it is more scattered, but I have never seen it at either end of the body. Although the most careful examination fails to detect any movement in the hyaline substance of the crescent, yet the existence of such may be inferred from the very positive movement which the pigment granules undergo. Fig. 7, a, b, c, represents these alterations; changes in form are exceptionally seen, as shown at Fig.8 (1,2,3). A crescent became, within an hour, an ovoid body.
Sketch 1 was made at 9.40, 2 at 10.10, and 3 at 10.30 p.m. The outline of these bodies is very clear and defined. Ovoid, elongated and rounded forms of identical structure are also met with, but the crescents predominate. The number is variable, from one or two in a slide, to six or eight in the field of the 1-12th im. Though almost always free, they occur sometimes in the interior of a corpuscle, indicating, doubtless, the mode of development (Fig. 8, a and b).
(b) The Rosette Form.—In six instances there were rounded bodies,a little larger than red corpuscles, with a dimly granular protoplasm, and in the centre a rosette of pigment (Fig.9). Some of these appeared
to be enclosed in a delicate membrane, others were free. In six cases remarkable changes were seen in these forms, of the nature of segmentation. Thus Fig.10, a, represents one of these as seen at
6 p.m., September 4th. At 6.10 (b) there were distinct indications of segmentation in the finely granular protoplasm. At 6.30 (c) this had resulted in the formation of twelve or fifteen rounded bodies clustered about the central pigment, and still enclosed in the sheath. At 7.40 (d) the shell had burst, and given exit to the small corpuscles, which presented a tiny speck at or about the centre. At 10.40 they had not undergone any material change. In Case 60, one of quartan ague, this phenomenon was repeatedly observed. The development of the rosette form can, I think, be traced from the intra-cellular pigmented bodies, which increase in size until the entire corpuscle is filled. In some instances the body was surrounded by the remnant of the red corpuscle, in others there was no trace of it. The pigment granules gradually collect in the centre of the body in a more or less distinct rosette. I thought these changes had been overlooked by the writers on this subject, but I find that Golgi[8] has given a very full description of them, and has beautifully figured the development of the rosette form from the intracellular pigmented bodies. He has followed the process of segmentation with much greater detail than I have been able to do.
(c) Flagellate organisms.—Two or three years ago, when I first read Laveran's papers, nothing excited my incredulity more than his description of the ciliated bodies. It seemed so improbable, and so contrary to all past experience, that flagellate organisms should occur in the blood. The work of the past six months has taught me a lesson on the folly of a scepticism based on theoretical conceptions, and of preconceived notions drawn from a limited experience. Flagellate bodies were seen in seven cases, never in great numbers, usually only one or two in a slide. They are smaller than red blood-corpuscles, of ten not more than half the size. A specimen in one case was equal in one diameter to a red corpuscle lying near it. They are round, ovoid, or pear-shaped; the protoplasm finely granular, and in every instance contained pigment, usually central, which often displayed rapid Brownian movements (Fig. 11). The flagella are variable in
number; one, three, and four were noted in different specimens. The length, as closely as could be estimated, was two or three times that of the body. They are exceedingly delicate, gently tapering, and, except in one instance, I could not determine the existence of a small terminal knob, figured by Laveran. The movement is exceedingly active, and the lashing of the long filaments may be sufficiently strong to drive away the corpuscles in the vicinity. The undulatory movement caused by the play of the filament over the surface of a group of corpuscles may attract the attention of the observer before he sees the cilia. The motion does not persist long, in none of the specimens which I examined, for more than half an hour. In one instance, the flagella disappeared in the short interval between two observations, but I could not determine what became of them. I have not seen the free-swimming cilia described by Laveran, but Dr. Councilman tells me that he has confirmed this observation. I have not been able to discover either nucleus or vacuoles in the flagellate organism. Slight, irregular changes in outline occur, due to slow movements in the protoplasm.
(d) Small, round, pigmented bodies, from one-fourth to one-half the size of a red corpuscle, were not uncommon in some cases (Fig. 12).

Usually, they remained unchanged, but, in several instances, they showed amœboid movements. The smaller ones about equal in size the products of subdivision of the rosette form.
Before proceeding to discuss the nature of these bodies and their relation, I will briefly refer to the condition of the blood-corpuscles.
The red corpuscles showed no other notable alteration save that already described. The pigmented organism evidently destroys the vitality, and consumes the hæmoglobin, for the affected cells become pale, often spherical, and, finally, are reduced to the condition of mere shells except in cases of pronounced anæmia, the variations of the corpuscles in size and outline were not great. The colourless corpuscles were in some cases increased in number, and in very many instances contained dark granules. In several specimens, they were observed to contain the pigmented organisms. In Case 40, a crescent had been included (Fig. 13), and, in Case 51, the process of inclusion
of two free pigmented bodies was watched during half an hour (Fig. 14). The blood-plaques were, as a rule, scanty, even when the anæmia was pronounced. No pigment was seen in them.
Types of Malaria Studied.—Of the seventy cases examined, a majority were instances of ordinary intermittent fever, chiefly quotidian and tertian, with two quartan cases. There was one case of remittent fever, one of comatose pernicious malarial fever, and the remainder were cases of malarial cachexia or chronic paludism, with occasional outbreaks of fever, with or without chills. In all of the cases, with the exception of seven, one or other of the forms above described was found in the blood.
Relation of the Forms to the Varieties of Malaria.—The pigmented amœboid bodies are met with in both acute and chronic cases, but they may be said to be specially characteristic of the more acute manifestations of the disease. In recent examples of quotidian or tertian ague which had not been under treatment, the amœboid intra-cellular forms were almost invariably present. I will refer subsequently in detail to the cases in which they were not found. The hyaline non-pigmented forms, and the vacuoles containing solid bodies, also occur in the acute cases; indeed, these latter forms were the only alterations noted in several instances. Thus, in Case 29, a man aged 48 was admitted to the Philadelphia Hospital September 27th, in a chill. He had had a paroxysm ten days before, and had suffered with malaria several years previously. The blood examined during the hot stages showed no pigmented bodies, but numerous corpuscles containing the vacuoles shewn in Figs. 5 and 6. The chills occurred on the 28th, 29th, 30th, and October lst; and each day the blood was carefully examiined, without finding other bodies than those in the vacuole or hyaline spaces. On October 1st, the patient began with ten grains of quinine twice a day, which was continued for five days. He had no chill after October 1st. On the 7th there were crescents in tolerable numbers, which persisted until the 27th, the date of the last examination.
The crescents appear to be associated with the more chronic forms of malaria, or with acute cases which have been under treatment for some time. Of eighteen cases in which they were present, in twelve there was a history of infection lasting from six weeks to six months. In many, the cachexia was marked, and the spleen greatly enlarged. In six instances the attacks were recent—under a month; but in every one of these cases quinine had been taken. As a rule, the crescents occur red alone in the blood; but there were cases observed in which the pigmented amœboid bodies, the rosette form, and the flagellate organisms, were also present. I did not find the crescents in any recent cases of intermittent fever which had not been under treatment.
The rosette form, with its peculiar segmentation, occurred in six cases, and always in association with the amœboid intra-cellular bodies. Case 31: tertian ague, examined in fourth attack; no medicine. Case 33: quotidian for seven days. Case 37: quotidian for six weeks, anæmic, and had a large spleen; took quinine one day. Case 39: quotidian for seven days. Case 58: quotidian, on and off, for six weeks, then stopped; now daily chill for a week. Case 60: quartan for three weeks. I have noted these details, as this form has not been much studied, and as Golgi seems inclined to ascribe to it an important connection with the development of the paroxysm. It was only observed in acute cases which had not been under treatment.
The flagellate organisms were present in seven cases, six of which were chronic forms, and one an acute case of three weeks' duration.
The small free pigmented bodies were very variable in numbers; they seemed more abundant in the chronic forms with cachexia.
Relation of those Forms to the Paroxysm.— Very many observations were made with a view of determining whether these organisms bore any definite relation to the remarkable periodic attacks which characterise acute malaria. For this purpose, in typical cases, examinations were made in the intervals of, just before, and in each stage of, the paroxysm. The results may be thus stated: there were instances, particularly if recent, in which the amœboid organisms were decidedly more numerous and larger before and during the paroxysms than in the intervals; there were others in which the number during the chill and hot stage was so small, that examples were very hard to find; in others again, slides taken before the attack and during each stage were negative, and yet insubsequent paroxysms the bodies were present in the blood. I think, on the whole, that the pigmented bodies in the red corpuscles are more numerous before and during an attack, but the difference is by no means striking, and I have repeatedly had to search long in slides prepared during a paroxysm for a single example. In acute cases which have lasted some weeks, and have had no medicine, the amœboid bodies have seemed to be quite as abundant at one time as another. Nor have I been able to see any special difference in the form of the bodies just before or during the chill, though in the early days of the attack they may be small and less distinctly pigmented, or indeed may present, as in Case 29, already referred to, the appearance of vacuoles containing small solid bodies.
The remarkable segmentation of the rosette form was in each instance met with during the paroxysm, and Golgi claims to have traced in five cases a series of changes corresponding to the stages of the attacks. In the intervals, the pigmented bodies gradually increase in size until they fill the affected red corpuscles, and finally the pigment collects in the centre, as shown at Fig. 9. The process of fission coincides with the onset and course of the paroxysm, and by the time of its conclusion the rosette forms disappear. In Case 60—a quartan ague—an attempt was made to follow these changes, with the following result. The patient, a lad of 18, had had malaria, on and off, for a year, but for three weeks before admission the chills had been recurring with regularity. On Saturday, the 6th, the blood was examined in the chill. The red corpuscles contained many large pigmented bodies, and the rosette forms were numerous, many in process of subdivision. On the 7th and 8th, he was free from fever, and the most careful examination of the blood failed to detect any forms but the ordinary pigmented intra-cellular bodies. They did not seem more numerous on the evening of the 8th than they were on the 7th. On the 9th, hourly examinations of the blood were made between 11a.m., when the fever began, and 4p.m. in the first two slides, there were very many pigmented bodies with the granules becoming concentrated, some with typical rosettes and a few in course of segmentation. In the specimens taken during the afternoon, the process of division was readily traced, and there were many of the small bodies in the field. On the 10th the note is: "No free bodies, all intra-cellular, tolerably numerous; no rosettes; no segmentation." On the 11th, several examinations were made, and then note reads, "absolutely none, save pigmented forms in the red." On the 12th, the slide at 8a.m. showed large number of pigmented bodies, some with the granules irregularly arranged, other with distinct rosette. Fever began at 12a.m. Throughout the paroxysm, hourly examinations were made; rosette forms were abundant, and segmentation active. On the 13th and 14th, the ordinary forms were present, and in the paroxysm of the 15th, the segmenting bodies were again seen. the development of pneumonia interrupted the observations. It is worth noting that in this case the onset of the paroxysms was marked by an outbreak of the most intense urticaria. Blood and lymph from the wheals did not show any special changes.
Certainly the segmentation seems associated in some way with the paroxysm in these cases, but unless our observations have been faulty or very incomplete, there are many others in which there are no such changes in the attack. It is a point, however, to which the attention of observers should be carefully directed.
The crescents appear, as already stated, to be confined to the more chronic cases, or to those which have had treatment. They may persist for weeks or months. Thus in Case 56—a patient had irregular fever with what he called dumb chills, which had lasted for a month—for three weeks there was fever without chills, the temperature rising on some occasions to 103°. The crescents were numerous, and were not associated with other forms. With this his general condition was good, and he did not look anæmic. Under arsenic he improved, and the fever subsided, but the crescents were still in his blood six weeks from the date of the first observation.
Genuine paroxysms may occur in these chronic cases without the development of other forms than the crescents. This observation was repeatedly made in Case 25, a man with irregular malaria of many months' duration and occasional severe chills. The flagellate organisms did not seem to have any special relationship to the paroxysm, but they were so rarely seen that my observations on this point are not of much value.
Influence of Medicines on the Organisms.—Quinine invariably caused the pigmented bodies to disappear. In acute cases, which were usually studied during two or three paroxysms before the administration was begun, this observation was repeatedly confirmed. In a few days the corpuscles were entirely free; in several instances, the crescents appeared before the blood became normal. For example, Case 46 had his first chill on October 1st, and a daily recurrence until the 10th, when he came under observation. The pigmented bodies were abundant, and continued so on the 11th and 12th, when the temperature rose in the paroxysm to 105°. Quinine (twenty grains) was given on the morning of the 13th (which broke the chill), and repeated on succeeding days. The bodies were present on the 13th, and a few on the 14th. They were not found on subsequent days. In less acute cases the action of the quinine did not seem to be so prompt, and the crescents did not disappear so rapidly under its use. Certainly, in recent cases this medicine acts as a positive specific against these organisms, just as it does against the malady itself. Arsenic does not appear to influence the pigmented intra-cellular bodies. In a chronic case, without chills, but with irregular fever, the crescents persisted for over five weeks, although the patient had improved in general health and vigour, and was no longer anæmic. Thallin and antifebrin were given in some cases without any noticeable results. As is well known to practitioners in malarial regions, there are cases of intermittent fever which subside without special treatment. I have had several patients in whom, without any quinine, the chills stopped or recurred very irregularly. In Case 66, the crescents appeared in the blood, which at first contained only the intra-cellular forms.
Cases examined with Negative Result.—As before stated, there were eight instances of apparently true malaria in which the organisms were not found, and to these I shall now briefly refer. I would remark, in the first place, that we cannot always rely upon one, or even two, examinations of the blood for these bodies. They may be very scanty, or they may be present at one examination and absent at the next. For example, Case 41, a young man, aged 26, was admitted with a temperature of 104°. He had been cranberry-picking in New Jersey, and had been ill for a week with fever and indefinite pains, but no chills. He was so very dull, that as the fever persisted, typhoid was suspected, although, as a cranberry-picker, malaria was first thought of. The blood was examined on three occasions with negative results, but on the fourth observation, five days after admission, and when the temperature had fallen to normal, crescents were found, which continued in the blood until he was thoroughly cinchonised. The cases are as follows:
Case 10. Child, aged 5; chills and fever in Maryland nine months ago, occasional chills since, the last two weeks ago; spleen 4 inches vertical diameter; had taken quinine, none recently. One examination.
Case 11. Man, aged 19; never malarial before. Four distinct paroxysms. Slides examined from fifth and sixth, taken in cold, hot, and sweating stages. No quinine. I did not see the case subsequently.
Case 20. Man, aged 40. First attack six months ago. Chills on and off for past three months. Blood examined three days after last chill. Had taken quinine for two days. Spleen enlarged.
Case 21. Man, aged 28. Examined on 17th, first chill on September 6th; four since. On 14th, took quinine grs. xxx, and has had gr. x. t. i. d. since.
Case 26. Man, aged 35. Chills for three weeks, at first quotidian, latterly tertian. Had taken medicine, but did not know the nature of it. Was admitted on 24th. Two examinations, negative; pigment in white corpuscles. On 25th quinine was given. Three subsequent examinations, without result.
Case 28. Man, aged 60. Admitted on 14th. Well-marked chills for eight weeks; had one when he came in, and four after. Blood examined on 28th, two slides. He had had quinine gr. xx each day since admission.
Case 38. Man, aged 70, resident of the almshouse for six years. First chill on 2nd, second on the 5th, third on 6th, when blood was examined, two slides.
Case 52. Man, aged 25. Chills and fever for six days. Blood examined in chill, and on the following day. Had had quinine.
Thus, in five of these cases quinine had been taken, and they may be counted out. In Case 10, the child was brought from the country, and only one examination was made. Case 11 was undoubtedly a case of quotidian ague, and the examination of slides taken from each stage of the fifth and sixth paroxysm was negative. I did not see the patient, and further examinations were not made. In Case 38, the bodies were not found on two occasions. This man also could not be followed, and I do not know his subsequent history.
The importance of excluding other causes for the paroxysmal chills was well illustrated by a case under the care of my colleague, Dr. J. H. Musser, which we regarded as one of malaria, but in which the pigmented bodies could not be found. The man had had chills on and off for several years; of late, the attacks had been more frequent and recurred more regularly. Quinine in medium-sized doses had no influence, but very large doses appeared to control the paroxysms. Their recurrence excited suspicions, and the discovery of pus in the urine, with decided pain on deep pressure in the lumbar region, indicated a more probable cause for the irregular chills.
Nature of the Organisms.—It is very evident that we are dealing here with structures unlike any others which have been described in human blood, and with bodies which have no relation whatever to the spirilla, micrococci, and bacteria of certain acute diseases. I would call attention to the remarkable unanimity in the description of these parasites by Laveran, Richard, Marchiafava and Celli, Councilman, Golgi, and myself. Laveran's original description is well-nigh complete, and subsequent workers have done little else than confirm his results, though to Marchiafava and Celli is due the credit of insisting upon the amœboid character of the intra-cellular form. Before discussing the relation of the forms to each other, it will be necessary to take a brief review of cognate organisms occurring in the blood, upon which recent investigations throw an important light.
It has been known for some years that hæmatozoa exist in the frog; one form, a flagellate organism, the Trypanosoma sanguinis, described by Grubyin 1843, is a well recognised monad; a second, the Drepanidium ranarum, of Lankester, is evidently a gregarine, possibly a larval form, as he suggests.[9] Having been long familiar with these bodies,[10] which were very abundant during several winters in the frogs in my labaratory at Montreal, I was at once struck with an apparent similarity to them of the forms found in malarial blood. The crescent-shaped body in particular resembles strongly certain of the gregarines, and I thought it possible that we had here an instance of a sporozoon becoming flagellate at one stage of its development as Rivolta affirms may be the case. I soon discovered, however, that there were other observations on hæmatoza which bore more directly on the subject, and rendered possible a more likely explanation. Mitrophanow,[11] in 1883, announced the discovery, in the blood of the carp and of the mud-fish, of parasites belonging to the flagellate infusoria. A description of these forms need not detain us, further than to note that they were polymorphic, and one stage was represented by an amœboid body without flagella.
In a report published by the Panjab Government, December 3rd, 1880, and in the Veterinary Journal, London, 1881-82, my friend, Dr. Griffith Evans, described a new and very fatal disease known as surra, which prevailed among horses, mules, and camels in India, and in which he discovered a parasite in the blood during life. At first Evans believed it to be a spirillum, but subsequently came to the conclusion that it was a much higher organism. His observations have an important bearing on the question of the parasites in malaria. In 1885, Veterinary-Surgeon Steel published "An Investigation into an Obscure and Fatal Disease among Transport Mules in British Burma," which also proved to besurra. A careful clinical investigation of the disease led to the conclusion that it was a true relapsing fever, very similar to recurrent fever of man. Steel found the parasite described by Evans in all cases, and determined that it appeared as the temperature rose and disappeared in the intervals between the paroxysms. He regarded it as a true spirillum, and named it Spirochceta Evansi. Both Steel and Evans found the disease readily communicable to dogs, horses, and mules, either by inoculation or by ingestion. Recently, on the return of Dr. Evans from India, he placed material from thesurradisease in the hands of Dr. Crookshank, who has made an elaborate report,[12] confirming Dr. Evans's view that the organism is not a spirillum, and states that the parasite is morphologically identical with the hæmatozoa described by Mitrophanow in the carp and mud-fish. In 1879, Lewis[13] described certain parasites in the blood of rats in India; and, again, in 1884,[14] he more fully discussed the question, and spoke of the identity of the organism with that found in the surra disease. Crookshank, in the paper just mentioned, gives the results of his investigations on the blood of European rats, 25 per cent of which he finds infested with Lewis's parasite. It is a flagellate organism, with an undulating fin-like membrane, and is highly polymorphic. Crookshank has distinguished "globose, angular, non-filamentous, bi-flagellate, semi-circular, and disc forms;" the latter represent the encysted stage. This organism is believed to be morphologically identical with the surra parasite and with Mitrophanow's hæmatozoa.
In the Biologisches Centralblatt, 1885, Professor Danielewsky, of Charkoff, makes an important contribution to the subject. He states that Trypanosoma, the well known flagellate organism of frog's blood is polymorphic, and occurs in an amœboid form, and also produces spores; and, further, he has found in the red blood-corpuscles of birds a pigmented protoplasmic body, which subsequently appears in the plasma as a pigmented flagellate organism. In a later communication,[15] he suggests the identity of the pathogenic blood parasites of man with the hæmatozoa of healthy animals, and refers specially to the similarity of the forms which he has found in birds to certain of those described by Laveran in malaria.
With this information, we are in a better position to discuss the relation of the forms described to each other, and the zoological position of the organism. It is evidently closely allied to the hæmatozoa just spoken of, and the facts which we know of their life-history enable us to assert, with greater confidence, that we are here dealing with the varieties of a highly polymorphic species, and not with two or three different organisms. The flagellate form is doubtless the adult condition; and it is interesting to note, in contrast to the hæmatoaoza of the rat and of the surra disease, the comparative infrequency of its occurrence. Laveran met with it ninety-two times in four hundred and thirty-two cases, and Councilman eleven times in eighty cases. The steps in development remain to be worked out. It seems clear, however, that the pigmented amœboid form may become transformed into a sporocyst (represented by the rosette form and its changes), or into an encysted body (resting form), the crescent. The gaps in our knowledge relate specially to the form and manner of entrance of the parasite in to the red corpuscle. Do the solid particles contained in the vacuoles (Figs. 5 and 6) represent the earliest stage? I think it highly probable that they do, and that they, with the hyaline unpigmented bodies, are the immature forms. The spore-like structures which result from the segmentation of the rosette form do not resemble the small solid bodies seen in the red corpuscles, but are rather like the tiny free pigmented forms which, in some cases, were abundant in the plasma. Of the latter, various sizes are found, and it is possible that from them the adult flagellate bodies arise. Golgi suggests that the spores, resulting from the segmentation, pass to the spleen, and there attack the red corpuscles, in which they develop into the amœboid forms. As at present the data are not available for a final decision, a further consideration of these points need not detain us. There is sufficient evidence to show that the various forms are only phases in the life-history of one of the flagellate protozoa, belonging to the order Flagellata-Pantostomata. Mitrophanow suggests a new genus, Hæmatomonas, to include the monad hæmatozoa; but Crookshank, who has carefully worked out the affinities of the parasites of the rat, the fish, and the surra disease, has referred them to the genus Trichomonas. The organism here described has not, however, the characteristic marks of a trichemonas; for it lacks the undulating fringe on one side and the caudal filament. Nor does it agree with the features of a Cercomonas; so that, meanwhile, until the true affinities are determined by an expert, its proper place seems to be the genus Hæmatomonas of Mitrophanow, which conveniently includes all monads parasitic in the blood. Thus: genus, Hæmatomonas; species, Hæmatomonas malariæ. Definition: Body plastic, ovoid, or globose, no differentiation of protoplasm, which contains pigment grains; flagella variable from one to four. Highly polymorphic, occurring in (1) amœboid form; (2) crescents, encysted form; (3) sporocysts; (4) circular, free, pigmented bodies. The name designates the natural affinities of the parasite, its habitat, and the conditions under which it occurs, on which grounds it seems preferable to that of Plasmodium malariæ, suggested by Marchiafava and Celli.
Relation of the Parasites to the Disease.—The same difficulty meets us here as in so many affection is in which micro-organisms have been found: Are they pathogenic, or are they merely associated with the disease, which in some way furnishes conditions favourable to their growth? As evidence of their pathogenic nature may be urged, with Laveran, the constancy of their presence, their absence, in other individuals in malarial regions, the destructive influence upon the blood-corpuscles, and their abundance in the graver forms of the disease. But even these considerations, weighty as they may appear, will not carry conviction to all, in the absence of experimental demonstration such as can be afforded in the case of certain pathogenic schizomycetes. Attempts to isolate and grow these hæmatozoa outside the body have failed. Marchiafava and Celli have shown that the inoculation of healthy persons with blood taken from a case of malaria is followed inavariable time by genuine ague paroxysms, in which the blood contains the parasites; but in regions where malaria is prevalent such experiments are not wholly free from objections. A series of negative observations on undoubted cases of malaria would be convincing. I lay no special stress on the three cases in which I did not find the parasites, as the patients were not followed from day to day with the accuracy necessary to give any value to the observations. It must be borne in mind that hæmatozoa are not uncommon in animals, and, as in the rat, do not appear to interfere seriously with the health of their hosts. Under these circumstances, the association of a specific form with a definite disease in an animal makes it all the more probable that the species is pathogenic. A further study of the surra disease is, particularly, to be desired with the new light which Evans and Crookshank have thrown upon it. the conditions under which the disease occurs, combined with its paroxysmal character, are so similar to those of malaria, that a full explanation of its pathogeny would have a very direct bearing upon the present question.
To my mind, two facts in connection with these hæmatozoa point significantly to their etiological association with malaria. First, the positive anatomical changes which can be directly traced to their action, changes upon which one at least of the most marked symptoms of the disease depends; I refer to the destruction of the red blood-corpuscles, which can be followed in all its stages, and is as well-defined an alteration of tissue brought about by a parasite, as any of which we know. The second fact is the action of quinine upon the parasites. The simultaneous disapearance of the symptoms of the disease and the hæmatozoa suggest that the specific influence of the medicine is upon the parasites, though it may be urged that the quinine, while curing the disease, simply removes the conditions which permit of their growth in the blood.
Practical Cocirations.—An interesting practical point is the diagnostic value of the presence of these bodies. There were six or eight cases in which the examination of the blood proved of great service in determining the existence of malaria. Some of these are worth mentioning. One of the first was a man aged 37, who had been under observation on three or four occasions with anæmia and an enlarged spleen. He had had three attacks of hæmatemesis. There was no history of malaria, and, from the gravity of the case, I was led to regard it as one of severe splenic anæmia. On his fourth visit, however, a careful examination of the blood revealed the presence of the parasites, and I gave, in consequence, a more favourable prognosis in the case, which has since been justified. In an instance of pernicious malaria admitted to the Philadelphia Hospital, under the care of my colleague, Dr. J. H. Musser, the diagnosis rested on the discovery in the blood of the characteristic changes in the corpuscles. To a third case, No. 41, I have already referred, and there were four or five other instances of chronic malaria in which the nature of the disease was determined by an examination of the blood. On the other hand, in many cases of suspected malaria, the absence of these bodies led to a more careful examination, and to the discovery of the cause of the chills and fever. Four of these were cases of phthisis with ill-defined physical signs; in a fifth, after several negative blood-examinations, the ague-like paroxysms were found to be due to aseptic pneumonia; in a sixth and seventh, renal disease was discovered. I feel confident that, in malarial regions,the examination of the blood will prove, in skilled hands, a most valuable aid in the diagnosis of many obscure cases.
Melanæmia.—These researches on malaria throw light on the formation of pigment in the blood and various organs in the chronic cases. Evidently the primary change is in the red blood-corpuscle, which is gradually destroyed by the amœboid form of the parasite. Every stage of this process can be readily traced, and these observations bear out the more recent views on the origin of the pigment in the blood itself. The pigmentary degeneration of the red corpuscles noticed long ago by Frerichs and by Kelsch,[16] was no doubt the same as here described. The gradual accumulation of the granules in the spleen, liver, and bone-marrow leads to the characteristic melanosis of these organs. I sought carefully for evidence of active interference with these parasites on the part of the white blood-corpuscles, but on only
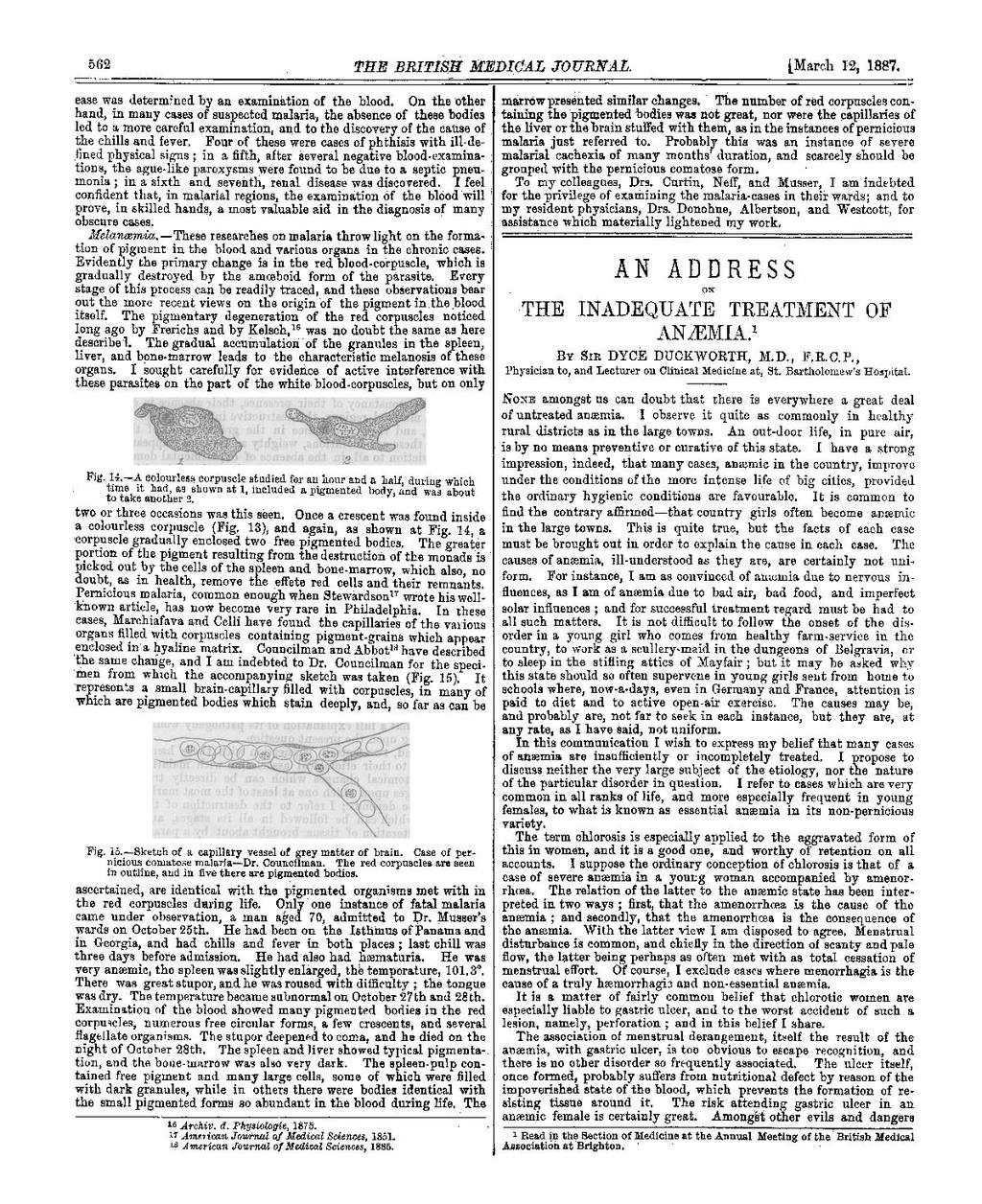
two or three occasions was this seen. Once a crescent was found inside a colourless corpuscle (Fig.13), and again, as shown at Fig.14, a corpuscle gradually enclosed two free pigmented bodies. The greater portion of the pigment resulting from the destruction of the monads is picked out by the cells of the spleen and bone-marrow, which also, no doubt, as in health, remove the effete red cells and their remnants. Pernicious malaria, common enough when Stewardson [17] wrote his well-known article, has now become very rare in Philadelphia. In these cases, Marchiafava and Celli have found the capillaries of the various organs filled with corpuscles containing pigment-grains which appear enclosed in a hyaline matrix. Councilman and Abbot[18] have described the same change, and I am indebted to Dr. Councilman for the specimen from which the accompanying sketch was taken (Fig.15). It represents a small brain-capillary filled with corpuscles, in many of which are pigmented bodies which stain deeply, and, so far as can be
ascertained, are identical with the pigmented organisms met within the red corpuscles during life. Only one instance of fatal malaria came under observation, a man aged 70, admitted to Dr. Musser's wards on October 25th. He had been on the Isthmus of Panama and in Georgia, and had chills and fever in both places; last chill was three days before admission. He had also had hæmaturia. He was very anemic, the spleen was slightly enlarged, the temperature, 101.3°. There was great stupor, and he was roused with difficulty; the tongue was dry. The temperature became subnormal on October 27th and 28th. Examination of the blood showed many pigmented bodies in the red corpuscles, numerous free circular forms, a few crescents, and several flagellate organisms. The stupor deepened to coma, and he died on the night of October 28th. the spleen and liver showed typical pigmentation, and the bone-marrow was also very dark. The spleen-pulp contained free pigment and many large cells, some of which were filled with dark granules, while in others there were bodies identical with the small pigmented forms so abundant in the blood during life. The marrow presented similar changes. The number of red corpuscles containing the pigmented bodies was not great, nor were the capillaries of the liver or the brain stuffed with them, as in the instances of pernicious malaria just referred to. Probably this was an instance of severe malarial cachexia of many months' duration, and scarcely should be grouped with the pernicious comatose form.
To my colleagues, Drs. Curtin, Neff, and Musser, I am indebted for the privilege of examining the malaria-cases in their wards; and to my resident physicians, Drs. Donohue, Albertson, and Westcott, for assistance which materially lightened my work.
- ↑ An address delivered before the Pathological Society of Philadelphia.
- ↑ Traité des Fivères Palustres Paris, 1884.
- ↑ Comptes Rendus, 1882.
- ↑ Fortschritte der Medicin, Nos. 14 and 24, 1885.
- ↑ Paper read before the Association of American Physicians, June, 1886.
- ↑ Councilman and Abbot, American Journal of Medical Sciences, April, 1885.
- ↑ Fortschritte der Medicin. 1885. No. 24.
- ↑ Sulla Infezione Malarica, Archivio per le Scienze Mediche, vol. x, No. 4, 1886.
- ↑ Quarterly Journal of Microscopical Science, vol. xxii.
- ↑ Canadian Naturalist. 1883.
- ↑ Biologisches Centralblatt, Bd. iii, p. 35.
- ↑ Journal of the Royal Microscopical Society. 1886.
- ↑ Quarterly Journal of Microscopical Science. 1879.
- ↑ Quarterly Journal of Microscopical Science. 1884.
- ↑ Centralblatt f. die Medicinischen Wissenschaften, Nos. 41 and 42. 1886.
- ↑ Archiv d. Physiologie, 1875.
- ↑ American Journal of Medical Sciences, 1851.
- ↑ American Journal of Medical Sciences, 1885.