twisted, bent, or otherwise strangulated, or its orifice may be blocked, so that the tube is distended with mucus which can find no outlet; or ulceration of tuberculous or malignant origin may occur. Inflammation started in the appendix is liable to spread to the peritoneum, and herein lies the gravity of the affection and the indication for treatment. The symptoms vary from “indigestion,” and slight pain and sickness, which pass off in a few short days, to an exceedingly violent illness, which may cause death in a few hours. Pain is usually first felt in the belly, low down on the right side or across the region of the navel; sometimes, however, it is diffuse, and at other times it is scarcely complained of. There is some fever, the temperature rising to 101° or 102° F., with nausea, and very likely with vomiting. The abdomen is tender to pressure, and the tenderness may be referred to the spot mentioned above. Some swelling may also be made out in that region. The attack may last for two, three or four days, and then subside. There are, however, other cases less well defined, in which the mischief pursues a latent course, producing little more than a vague abdominal uneasiness, until it suddenly advances into a violent stage. In some chronic cases the trouble continues, on and off, for months or even for years.
 |
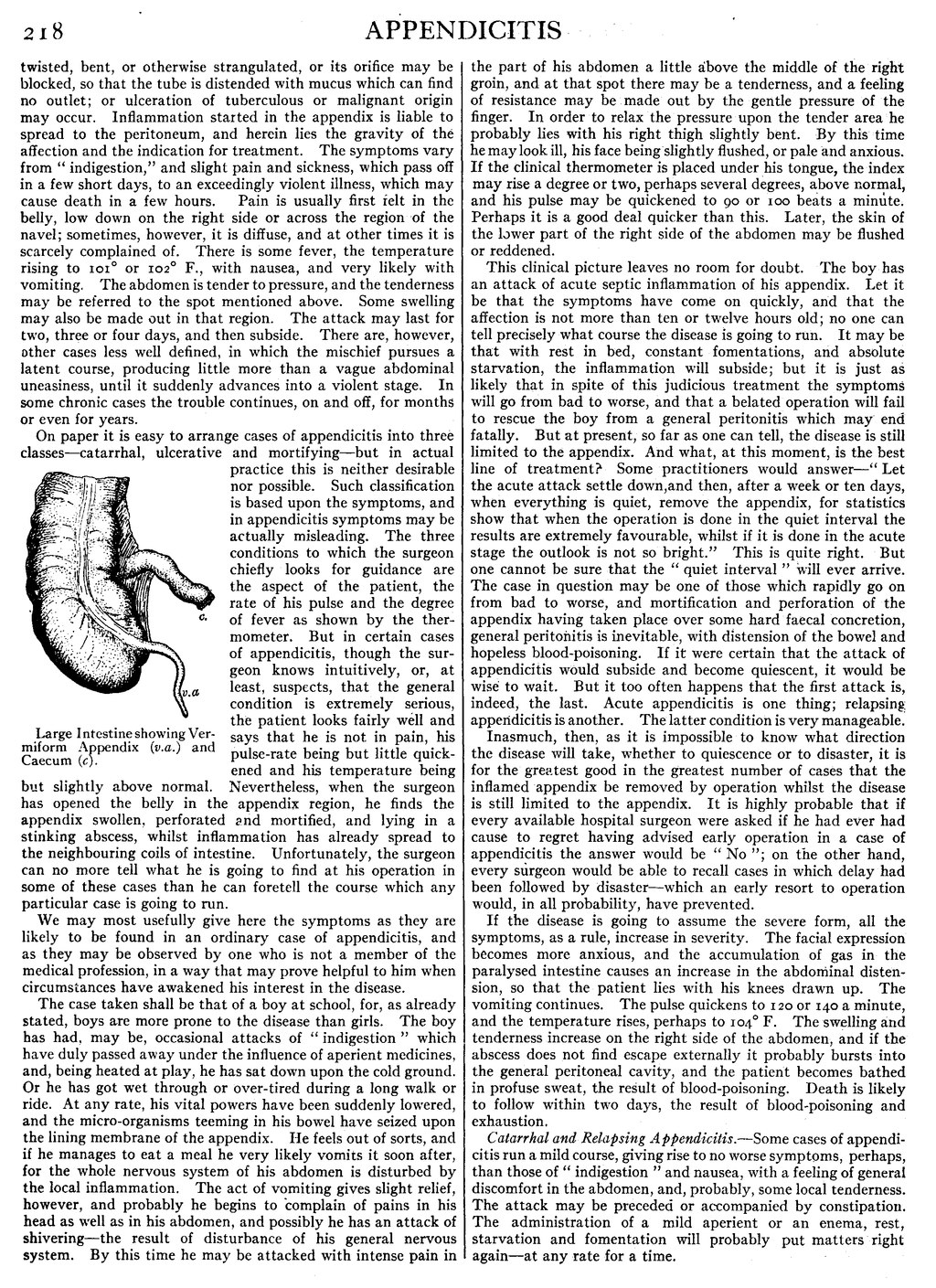
| Large Intestine showing Vermiform Appendix (v.a.) and Caecum (c). |
On paper it is easy to arrange cases of appendicitis into three classes—catarrhal, ulcerative and mortifying—but in actual practice this is neither desirable nor possible. Such classification is based upon the symptoms, and in appendicitis symptoms may be actually misleading. The three conditions to which the surgeon chiefly looks for guidance are the aspect of the patient, the rate of his pulse and the degree of fever as shown by the thermometer. But in certain cases of appendicitis, though the surgeon knows intuitively, or, at least, suspects, that the general condition is extremely serious, the patient looks fairly well and says that he is not in pain, his pulse-rate being but little quickened and his temperature being but slightly above normal. Nevertheless, when the surgeon has opened the belly in the appendix region, he finds the appendix swollen, perforated and mortified, and lying in a stinking abscess, whilst inflammation has already spread to the neighbouring coils of intestine. Unfortunately, the surgeon can no more tell what he is going to find at his operation in some of these cases than he can foretell the course which any particular case is going to run.
We may most usefully give here the symptoms as they are likely to be found in an ordinary case of appendicitis, and as they may be observed by one who is not a member of the medical profession, in a way that may prove helpful to him when circumstances have awakened his interest in the disease.
The case taken shall be that of a boy at school, for, as already stated, boys are more prone to the disease than girls. The boy has had, may be, occasional attacks of “indigestion” which have duly passed away under the influence of aperient medicines, and, being heated at play, he has sat down upon the cold ground. Or he has got wet through or over-tired during a long walk or ride. At any rate, his vital powers have been suddenly lowered, and the micro-organisms teeming in his bowel have seized upon the lining membrane of the appendix. He feels out of sorts, and if he manages to eat a meal he very likely vomits it soon after, for the whole nervous system of his abdomen is disturbed by the local inflammation. The act of vomiting gives slight relief, however, and probably he begins to complain of pains in his head as well as in his abdomen, and possibly he has an attack of shivering—the result of disturbance of his general nervous system. By this time he may be attacked with intense pain in the part of his abdomen a little above the middle of the right groin, and at that spot there may be a tenderness, and a feeling of resistance may be made out by the gentle pressure of the finger. In order to relax the pressure upon the tender area he probably lies with his right thigh slightly bent. By this time he may look ill, his face being slightly flushed, or pale and anxious. If the clinical thermometer is placed under his tongue, the index may rise a degree or two, perhaps several degrees, above normal, and his pulse may be quickened to 90 or 100 beats a minute. Perhaps it is a good deal quicker than this. Later, the skin of the lower part of the right side of the abdomen may be flushed or reddened.
This clinical picture leaves no room for doubt. The boy has an attack of acute septic inflammation of his appendix. Let it be that the symptoms have come on quickly, and that the affection is not more than ten or twelve hours old; no one can tell precisely what course the disease is going to run. It may be that with rest in bed, constant fomentations, and absolute starvation, the inflammation will subside; but it is just as likely that in spite of this judicious treatment the symptoms will go from bad to worse, and that a belated operation will fail to rescue the boy from a general peritonitis which may end fatally. But at present, so far as one can tell, the disease is still limited to the appendix. And what, at this moment, is the best line of treatment? Some practitioners would answer—“Let the acute attack settle down, and then, after a week or ten days, when everything is quiet, remove the appendix, for statistics show that when the operation is done in the quiet interval the results are extremely favourable, whilst if it is done in the acute stage the outlook is not so bright.” This is quite right. But one cannot be sure that the “quiet interval” will ever arrive. The case in question may be one of those which rapidly go on from bad to worse, and mortification and perforation of the appendix having taken place over some hard faecal concretion, general peritonitis is inevitable, with distension of the bowel and hopeless blood-poisoning. If it were certain that the attack of appendicitis would subside and become quiescent, it would be wise to wait. But it too often happens that the first attack is, indeed, the last. Acute appendicitis is one thing; relapsing appendicitis is another. The latter condition is very manageable.
Inasmuch, then, as it is impossible to know what direction the disease will take, whether to quiescence or to disaster, it is for the greatest good in the greatest number of cases that the inflamed appendix be removed by operation whilst the disease is still limited to the appendix. It is highly probable that if every available hospital surgeon were asked if he had ever had cause to regret having advised early operation in a case of appendicitis the answer would be “No”; on the other hand, every surgeon would be able to recall cases in which delay had been followed by disaster—which an early resort to operation would, in all probability, have prevented.
If the disease is going to assume the severe form, all the symptoms, as a rule, increase in severity. The facial expression becomes more anxious, and the accumulation of gas in the paralysed intestine causes an increase in the abdominal distension, so that the patient lies with his knees drawn up. The vomiting continues. The pulse quickens to 120 or 140 a minute, and the temperature rises, perhaps to 104° F. The swelling and tenderness increase on the right side of the abdomen, and if the abscess does not find escape externally it probably bursts into the general peritoneal cavity, and the patient becomes bathed in profuse sweat, the result of blood-poisoning. Death is likely to follow within two days, the result of blood-poisoning and exhaustion.
Catarrhal and Relapsing Appendicitis.—Some cases of appendicitis run a mild course, giving rise to no worse symptoms, perhaps, than those of “indigestion” and nausea, with a feeling of general discomfort in the abdomen, and, probably, some local tenderness. The attack may be preceded or accompanied by constipation. The administration of a mild aperient or an enema, rest, starvation and fomentation will probably put matters right again—at any rate for a time.